 By
By
A hospital can post a positive margin and still be weeks from a cash crisis. Shellie Shouse, a rural hospital CEO at Ohio County Healthcare who came up through reimbursement and revenue cycle, has seen the gap between accounting health and operating liquidity often enough to know the sequence that closes it.
That gap is the central problem for any CFO or VP of Revenue Cycle being asked to lead a turnaround. Margin is a story the income statement tells. Cash is what pays nurses on Friday and keeps the credentialing file moving. When Shouse talks about how she would walk into a struggling rural hospital tomorrow, she doesn't start with strategy. She starts with cash, then revenue cycle leakage, then leadership alignment. In that order.
This piece works that sequence as one argument. The thesis: distressed hospitals don't fail at vision. They fail at the order of operations.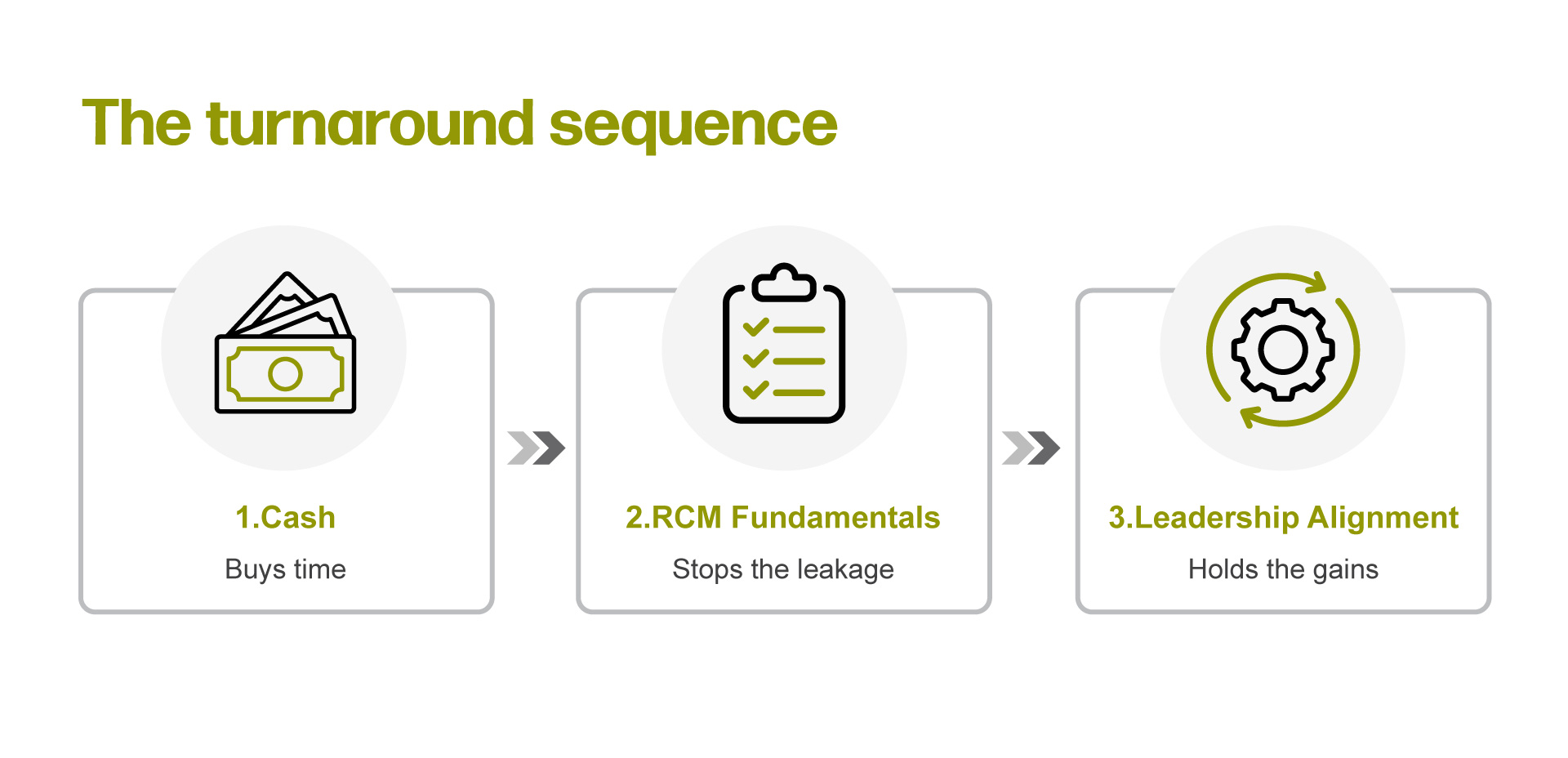
Cash Buys Time, Margin Buys Nothing
Shellie is direct about what the top CEO metric is, and it isn't margin.
“Cash. Specifically, sustainable operating cash flow,” said Shouse.
She continues: a hospital can report positive margins and still have cash problems. Cash provides flexibility to invest in people, facilities, technology, and new services. Everything else - AR days, denial rates, labor productivity, payer mix, operating margin - she watches as diagnostics that explain why cash is moving the way it is.
For an RCM leader, this reframes what the team is actually optimizing. Gross collections is not the headline. Days-to-cash is. A denial that drags on through a long appeal cycle is a worse outcome than a write-off you book early, because the first one ties up working capital while pretending to be revenue. Shouse's lens forces that distinction.
Her first move in a turnaround follows from this.
“First, I’d examine cash because cash buys time,” Shouse said.
Time is the asset that lets the rest of the work happen. Without it, the turnaround compresses into layoffs and service line cuts before anyone gets to the upstream fixes. With it, the second step becomes possible.
Where the Leakage Lives
Once cash buys time, Shouse goes after the revenue cycle. She is specific about the diagnostic set: AR days, denial trends, DNFB, point-of-service collections, and underpayment monitoring. She calls this the place where many hospitals unknowingly leave money on the table.
Each of those line items is a distinct capability question for the operator. AR days requires analytics access and exception management. Denial trends require denial intelligence and payer policy expertise. DNFB requires documentation governance and coding throughput. POS collections require patient access discipline. Underpayment monitoring requires contract analytics and the staffing leverage to actually work the variances.
How a given system acquires those capabilities - internal build, vendor partnership, managed services, or some hybrid - is downstream of recognizing that they have to exist somewhere in the operation. The point is that "fix the revenue cycle" is not an action item. The five items Shouse lists are.
Shouse also names a leakage source most RCM dashboards miss: provider onboarding.
“I’ve experienced in the past being in the revenue cycle, oh my, we did not know that physician was coming,” said Shouse. “And now we’re behind in credentialing, and that affects your payments.”
When provider recruitment and payer enrollment operate without a tight handoff, the revenue cycle can find out about a new physician only after claims start denying. That kind of disconnect between operational planning and reimbursement readiness is a cash problem hiding inside an internal communication gap.
Shouse's framing - that every operational decision has a financial consequence - applies most literally here. A recruiting decision becomes a cash decision when the enrollment file moves on time, and a write-off when it doesn't.
The Reason RCM Stays Underfunded
The reader's likely objection at this point: we know all of this. Why doesn't the investment follow?
Shouse has a clean answer.
“People notice a new building, a new physician, a new service line,” said Shouse. “They don’t necessarily notice clean claims, fewer denials, or improved collection process.”
This is the structural reason revenue cycle keeps getting pitched as a back-office function even when leaders intellectually know better. Clean claims don't get ribbon cuttings. Denial rate improvements do not show up in the local paper. Shouse observes that organizations can recover significant revenue by improving processes, reducing AR, improving front-end registration, and identifying underpayments - work that can create millions of dollars in value - and still struggle to be seen.
For an RCM leader, the implication is operational, not rhetorical. If invisible wins stay invisible, they don't get reinvested in. The work of the function includes translating those wins into language a board uses: liquidity runway, strategic capacity, risk reduction. Shouse's framing of board communication reinforces this. Boards work at the governance level. They want confidence that leadership understands the issues, has a plan, and is managing risk. Reporting raw AR days to a finance committee is operational detail. Reporting that AR compression has added cash on hand and funded a planned recruitment cycle is governance.
This is where most RCM presentations fail. They report metrics. They don't report consequences.
Why Leadership Alignment Is Third,
Not First
Shouse's third turnaround lever is culture and leadership alignment. She is explicit that even the best turnaround plan fails if leadership isn't pulling in the same direction.
The order matters. Cash first, because without it the building burns down while the team is workshopping values. RCM fundamentals second, because that is where the cash actually comes from in the medium term. Leadership alignment third, because sustaining the gains requires people who agree on what they're doing.
Shouse's broader leadership philosophy frames why this sequencing works.
“What I learned is that organizations improve through people and not spreadsheets,” Shouse said. “Financial results improve when employees understand the mission, when leaders are aligned, and when teams trust one another.”
She calls numbers outcomes, not causes. The point is not that culture work replaces operational work. The point is that operational fixes don't hold when the leadership team disagrees about what the operation is for. Denial reduction initiatives that lack alignment across the executive team tend to produce short-term improvement that doesn't sustain.
For the reader running a turnaround, the practical question is whether the executive team agrees on the diagnostic before the work starts. If cash is the scorecard, does the COO know that? If credentialing handoffs are costing money, does the CMO own the upstream piece of that workflow? If front-end accuracy is the leverage point, does patient access report into someone who treats it as strategic rather than clerical?
What RCM Leaders Should Take From This
Shouse's revenue cycle background is doing more work in her CEO seat than most boards recognize when they hire from finance. She describes revenue cycle as starting when the patient schedules and continuing until the account is resolved, touching access, scheduling, physicians, nursing, case management, HIM coding, billing, compliance, and finance. That breadth is why she sees credentialing as a revenue problem and cash as a culture problem.
The lesson for the reader is not that every RCM director should plot a path to the CEO office. The lesson is that the function has a system-wide vantage point most other operational seats don't, and that vantage point is wasted when revenue cycle is run as a billing department.
Three things follow:
- Reframe RCM internally as end-to-end, starting at scheduling. Front-end accuracy, eligibility, estimates, and credentialing are revenue cycle. Treating them as someone else's problem is how the leakage starts.
- Tie RCM performance discussions to cash, not collections. AR days, denial trends, DNFB, POS collections, and underpayment monitoring are the diagnostic set that explains cash movement. That is the language the CEO and the board care about.
- Quantify invisible wins. Clean claims, fewer denials, and faster cash realization don't market themselves. The function has to do that work, or it stays underfunded.
What Changes Monday
For a CFO or VP of Revenue Cycle walking into a distressed hospital this quarter, Shouse's sequence is the spine: cash first to buy time, RCM fundamentals second to stop the leakage, leadership alignment third to hold the gains.
Monday means pulling the cash position and building a near-term liquidity view before anything else. It means auditing the five items Shouse named - AR days, denial trends, DNFB, POS collections, underpayment monitoring - and adding credentialing cycle time as a sixth, because the provider onboarding handoff is where preventable cash disruption lives. It means asking, honestly, whether the executive team is aligned on what the turnaround is actually solving for.
This fiscal year means deciding how the underlying capabilities get acquired. Analytics access, denial intelligence, patient access discipline, contract management for underpayments, payer enrollment governance. These have to live somewhere in the operation. The form they take depends on the system's size, geography, and maturity. The capability does not.
Shouse's closing point is the one to carry into the next budget conversation: financial stewardship and mission stewardship are the same work. A rural hospital that runs its revenue cycle well has the cash to keep its doors open, recruit the next physician, and serve the community that depends on it. A rural hospital that doesn't, won't. The sequence isn't complicated. The discipline to follow it is.

